ABSTRACT
The use and popularity of both zirconia and lithium disilicate have increased dramatically over the last several years (Fig. 1). In fact, if current trends hold1 it is entirely possible that that the escalating use of both zirconia and lithium disilicate will soon lead to the demise of traditional PFM’s. This article will focus specifically on zirconia.
Zirconia has many positive attributes not the least of which is high strength. In fact, the flexural strength of monolithic zirconia crowns can be anywhere from five to well over 10 times that of conventional PFM’s.2-4 Likewise, the fracture toughness (ability to resist crack propagation) of zirconia is significantly higher than both lithium disilicate and PFM restorations.5 In addition,
zirconia can be bonded or conventionally cemented, is very wear-friendly to opposing tooth structure when properly polished, is compatible with CAD-CAM technology, and can be used in the monolithic form to maximize strength or as a supportive substructure and layered with various ceramics to optimize esthetics. This article will focus on just what zirconia is, its advantages and disadvantages, recent improvements in optical properties, misconceptions some may have, how to optimize the zirconia surface prior to placement, and various cementation options.
What is Zirconia?
Zirconia is often referred to as “white metal” or “white steel”. This terminology may have originated with the introduction of razor-sharp zirconia knives used as cutlery with blades that are typically harder and more corrosive resistant than those of their steel counterparts (Fig. 2). Of course, zirconia is not steel. In fact, it is not even a metal. Zirconia is the oxide of the element zirconium (element 40 in the periodic table). While the element zirconium is a tough hard silvery white metal (Fig. 3) its oxide, the zirconia we use in dentistry, is not. Zirconium is not found in nature in its pure elemental form. It exists combined with other elements forming minerals such as zircon (ZrSiO4) and baddeleyite (mostly ZrO2). These and other minerals are mined, refined, and purified through a number of complex physical and chemical processes to produce zirconium oxide powder (ZrO2) (Fig. 4). This powder (a polycrystalline ceramic) can be shaped, pressed, and fully or partially sintered to create zirconia pucks and blocks (Fig. 5) that can be milled using CADCAM technology to create zirconia dental restorations and supporting frameworks.
Types of Zirconia
Zirconia exists in three distinct temperature and pressure dependent crystalline configurations or phases (monoclinic, tetragonal, and cubic). At normal temperatures and pressures zirconia exists in the monoclinic crystalline form. While this is the most stable configuration of zirconia it lacks the physical properties required for dental use. When heated to approximately 1170°C the monoclinic powdered form of zirconia will coalesce into a solid (sintering). During this process the zirconia crystals undergo a phase transformation from the monoclinic to the tetragonal crystalline configuration (Fig. 6). This form of zirconia is very strong, biocompatible, corrosion resistant, can be milled, and has the physical properties necessary for use as a dental restorative or supporting structure. When further heated to approximately 2,100°C another phase transformation occurs and the tetragonal crystals transform to the cubic crystalline configuration forming a very hard, translucent, and somewhat brittle
Zirconia Conundrums
One of the problems with the tetragonal form of zir- conia used in the fabrication of dental restorations is it is not inherently stable and readily converts back to its weaker, more stable, and lower energy state monoclin- ic crystalline form. Various dopants such as yttrium oxide (Y2O3) and aluminum oxide (Al2O3) are add- ed in very small amounts to stabilize the tetragonal crystalline lattice as well as modify optical properties. This so called “yttria-stabilized zirconia” is in fact, not entirely stable. It is actually “metastable” meaning that given the right conditions the tetragonal crystals can convert back into their monoclinic configuration.
On a small scale this is actually a desir- able property as it makes zirconia resistant to crack propagation via a property called transformation toughening. Simply stat- ed, as a crack is initiated on the zirconia surface and begins to propagate there is a localized conversion of the tetragonal crystals around the advancing crack front back into the monoclinic form. This re- sults in a localized volumetric expansion of the crystals (around 4%) surrounding the crack essentially compressing and sealing the defect and mitigating further crack advancement. So, on a small scale the metastable nature of zirconia can be a positive attribute due to transformation toughening.
However, on a large scale it can be a negative as excessive tetragonal to monoclinic phase transformation can weaken overall assembly strength po- tentially leading to catastrophic failure. Indeed, in the early part of this centu- ry thousands of Prozyr zirconia femoral heads (used in hip replacement surgery) were recalled due to numerous instances of spontaneous fracturing of the zirconia femoral heads within 27 months of place- ment (expected lifespan was at least 10 years). The failures were attributed in part to minute changes in processing tempera- tures during manufacture that resulted in excessive tetragonal to monoclinic phase transformation over-time.9-11 These fail- ures highlight the importance of using zirconia produced by reputable manufac- tures (all zirconia is not created equally).
To take full advantage of the physical properties of zirconia it makes sense to use them as full contour monolithic res- torations whenever possible. That is, to avoid layering or pressing ceramics over zirconia (as is often done to optimize esthetics) because the layering ceramic, along with the interface between the zir- conia and layered ceramic, are weak links in the restorative assembly. In addition, monolithic zirconia restorations that can be milled full contour keep costs low as no additional time is required for layer- ing by a ceramist. While high strength monolithic zirconia restorations make sense, esthetics can be an issue in the an- terior regions of the mouth where the in- herently high value and stark white color of some monolithic zirconia restorations, coupled with a lack of translucency and fluorescence, can make them unsuitable when optimal esthetics is required. The esthetics of monolithic zirconia has im- proved significantly in recent years with the introduction of so-called “translu- cent” zirconia. Manufacturers employ a number of techniques to improve the translucency of zirconia including reduc- ing grain size, reducing alumina content, modification of processing and pressing techniques, altering sintering times and temperatures, and manipulating dopant levels to increase the percentage of the more translucent cubic crystals relative to the more opaque tetragonal crystals.
Sandblasting Zirconia Prior To Placement
It is the author’s strong opinion that the zirconia surface should be particle abraded (sandblasted) prior to placement no matter what type of conventional or resin-based cement is used. There is significant sup- port in the literature for this recommen- dation.15-18 While there is some concern that sandblasting has the potential to in- duce surface and subsurface cracks and/or
defects that could reduce physical proper- ties19,20, the author is unaware of any stud- ies that demonstrate this to be a clinical problem assuming appropriate blasting pressures, particle types, and particle sizes are utilized. In fact, some studies found that sandblasting actually increases the flexural strength of zirconia (due to trans- formation toughening).12,21 Sandblasting zirconia is useful in terms of cleaning the target surface of impurities, increasing surface roughness and surface area, raising surface energy, improving the bond to zir- conia primers and adhesives, and generally optimizing the surface prior to bonding or conventional cementation.22 Having said this, the term “sandblasting” is very am- biguous. Sandblast with what exactly? At what pressure and distance? The general consensus among researchers and opinion leaders is that traditional high strength zirconia (3-4 mol% yttria concentration) can be safely and effectively sandblast- ed with 30-50 micron aluminous oxide (Al2O3) using a blast pressure of 1.5-2.8 bar (approximately 20-40 psi) from a dis- tance of 1-2 cm and for a duration of 10-20 seconds.18,23,24 In addition, some research- ers recommend the nozzle head be held at an angle of approximately 60 degrees.24 When dealing with translucent zirconia (5 mol% yttria concentration) that has a reduced capacity to undergo transforma- tion toughening, blasting pressures should be in the lower range (approximately 20 psi) to minimize any surface damage that could lead to a reduction in physical prop- erties. Burgess and McLaren have sug- gested using 50-micron silica glass beads as an alternative to harder aluminum ox- ide particles when sandblasting translu- cent zirconia.25 Their testing showed no reduction in the physical properties when glass beads were used. Additional testing is needed to confirm and refine optimal protocols for sandblasting both translucent and high strength zirconia.
As far as when to sandblast, the au- thor prefers to sandblast the intaglio sur- face of zirconia restorations after try-in and any adjustments, and just prior to
conventionally cementing or adhesively bonding the restoration into place. In this regard, the author strongly recom- mends that dentists invest in a quality chair-side sandblasting unit (i.e. Micro- etcher II, Danville Materials) and dust cabinet with a built-in fan filtration unit (i.e. Microcab, Danville Materials). If the dentist does not have a sandblaster then the author recommends having the dental laboratory sandblast the resto- ration just before shipment. Of course, this requires a high degree of faith that the dental lab is sandblasting the zirconia correctly. Once the zirconia restoration is ready for placement dentists have several important decisions to make: 1) Should the restoration be conventionally cement- ed or adhesively bonded into place? 2) Should a separate zirconia primer such as 10-Methacryloyloxydecyl Dihydrogen Phosphate (10-MDP) be applied at some point after sandblasting? 3) Is it necessary to clean the zirconia surface before ce- mentation with alkaline solutions such as Ivoclean (Ivoclar) or ZirClean (BISCO)?
Are Alkaline Cleaning Solutions Necessary Prior to Zirconia Primer Application?
It is the author’s strong opinion that if you want to predictably and durably bond to zirconia with resin-based cements then it must be sandblasted and a zirconia primer placed. The primer can take the form of a separately applied solution that contains a phosphate ester zirconia prim- er such as 10-MDP (i.e. Z-Prime/BIS-
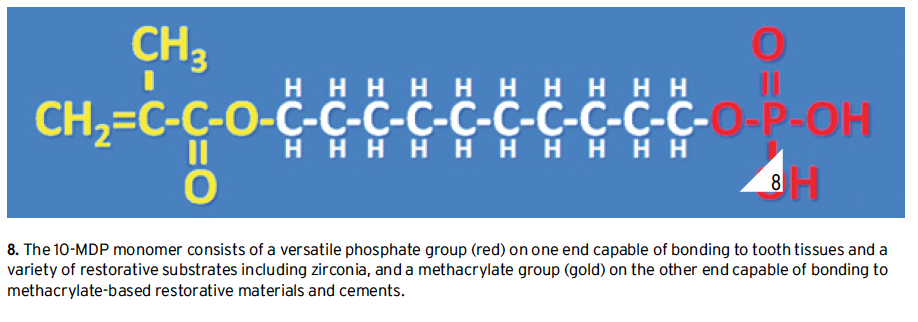
CO, Monobond Plus/Ivoclar, Clearfil Ceramic Primer Plus/Kuraray, various universal adhesives22, etc.) or by using a resin cement that incorporates a zirconia primer directly in its chemical makeup (i.e. PANAVIA SA Cement Plus Ku- raray, Unicem 2/3M ESPE). A recent study found that 10-MDP zirconia primers chemically interact with the zir- conia surface by both hydrogen and ionic bonding mechanisms.26 This chemical interaction requires that terminal phos- phate groups in zirconia primer mole- cules such as 10-MDP (Fig.8)can freely interact with reactive sites on the zirconia surface. Zirconia has a remarkable affin- ity for phosphate ions.27 This affinity ex- tends not only to the phosphate groups in zirconia primers but also to phosphate groups and ions that are inherent in sa- liva. When zirconia restorations are tried in and the intaglio surface is contaminat- ed by saliva, the phosphate ions from the saliva bind to, and occupy, the same reac- tive sites that zirconia primers require for chemical interactions. This competition for reaction sites significantly decreases the efficacy of zirconia primers and it is necessary to “free-up” these sites so zir- conia primers can function optimally. This can be accomplished by sandblast- ing the restoration after saliva contami- nation and/or the use of strongly alkaline cleaning solutions such as Ivoclean (Ivo- clar Vivadent) or ZirClean (BISCO). It should be pointed out that vigorous rins- ing with water, or the use of acetone and alcohol, is not effective in cleaning zirco-
nia surfaces that have been contaminated with saliva.28 Products such as Ivoclean and ZirClean essentially work by hav- ing a higher affinity for phosphate ions than does the zirconia itself. In effect, the cleaning agent chemically scavenges phosphate ions from the zirconia surface and in so doing frees up reaction sites that now become available for chemical inter- action with subsequently placed zirconia primers. If the dentist is sandblasting the zirconia restoration themselves (after it is tried in and just prior to placement), then the use of a separate cleaning agent is not necessary (but still an option) as the sandblasting alone is sufficient in terms of freeing up reaction sites. If the den- tist does not have a sandblaster, and had the dental lab sandblast the restoration before shipment, then the restoration SHOULD be treated with a cleaning solution such as Ivolean or ZirClean (af- ter it has been tried in and prior to prim- er application). To reiterate, studies show that the best way to treat saliva-contam- inated zirconia surfaces is by sandblast- ing and/or the use of strongly alkaline cleaning solutions such as Ivoclean or ZirClean.29,30 Two last important notes:
1) While phosphoric acid (H3PO4) is an effective cleaning agent for saliva-con- taminated silica-based ceramics (such as stacked porcelain and lithium disilicate), it is contraindicated for cleaning zirconia surfaces. This is because, just as in the case of saliva, the phosphate ions from the phosphoric acid remain bound to the zirconia surface (even after rinsing) and tie-up reaction sites required for chemical interaction with zirconia primers. 2) While silane is an effective primer for sili-effective for priming zirconia sur- ate ester primers such as 10-MDP).
Cementing and Bonding Zirconia Restorations
The fact is there is not one specific universal protocol to use when it comes to the placement of zirconia restorations. The optimal way to treat both the zirconia and tooth surfaces prior to placement is con- tingent on many factors including, the specific clinical conditions, how retentive the preparation is, the nature of the conventional or resin-based cement being used, the minimum occlusal thickness, whether the dentist or the lab sandblasted the zirconia, the type of zirconia being placed (conventional vs. translucent), and esthetics (will the color of the cement affect the esthetic result). As previously discussed and as a general rule, the author recommends that the in- taglio surface of all zirconia restorations be particle abraded (sand- blasted) and a zirconia primer placed (typically a phosphate ester such as 10-MDP). However, this is not true in every situation and the use of a separate zirconia primer is actually contraindicated or not necessary with some materials. As an example, Ceramir C&B (DOXA Dental) is a “bioactive” glass ionomer/calcium aluminate hybrid cement that is very hydrophilic in nature. Hydrophilic sur- faces generally interface well with other hydrophilic surfaces (“like likes like”) but are generally less or non-interactive with hydropho- bic surfaces. For example, water (hydrophilic) does not mix well with oil (hydrophobic). Properly sandblasted zirconia has a high energy hydrophilic surface. Once a zirconia primer is placed the hydrophilic surface becomes hydrophobic (Fig.9). This is advan- tageous when using methacrylate-based resin cements that are also hydrophobic but can be a detriment with hydrophilic non-resin containing materials such as Ceramir C&B. Indeed, there are a number of anecdotal reports of zirconia crowns loosening or falling out when a zirconia primer was used prior to cementation with Ce- ramir C&B. For those dentists using Ceramir C&B, the zirconia surface should still be sandblasted to optimize surface conditions, but a zirconia primer should NOT be used.32 Likewise, conven- tional glass ionomer cements (i.e. Fuji II/GC, Ketac CEM/ 3M ESPE) do not require the use of a separate zirconia primer.
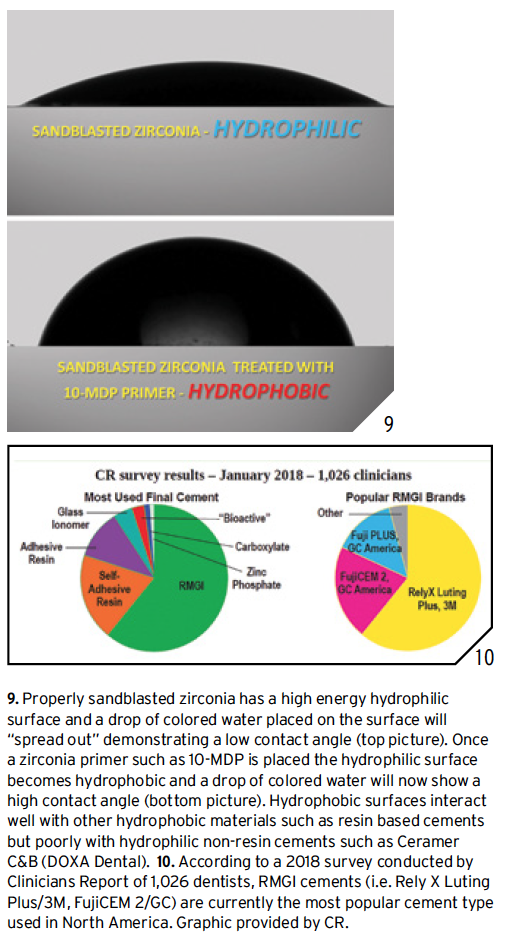
However, zirconia primers (i.e. Z-Prime, BISCO, Monobond Plus, Ivoclar) have been shown to increase bond strength of zir- conia to both RMGI33,34 and methacrylate based resin cements.35 RMGI (resin-modified glass ionomer) cements have many pos- itive attributes including good physical properties, low solubili- ty, some chemical bond to tooth structure, low film thickness, fluoride release, anti-microbial activity, good long-term clini- cal track record, and low incidence of postoperative sensitivity. Perhaps the biggest clinical advantages of RMGI cements is that they are very easy to mix, place, and clean. In fact, cement cleanup is generally much easier compared to resin cements, and this fact alone makes RMGI an attractive cementation option. Indeed, according to a 2018 survey of 1,026 dentists, RMGI cements (i.e. Rely X Luting Plus/3M, FujiCEM 2/GC) are currently the most popular cement type used in North America36 (Fig.10). The author personally considers RMGI to still be one of the best cementation options for high strength zirco- nia assuming the preparations have proper resistance and re- tention form and a minimum occlusal thickness of 1 mm or more. Even though studies appear to support the application of a separate zirconia primer after sandblasting to enhance the bond of RMGI to zirconia, the actual clinical relevance and benefit of this extra step is unclear and open for debate. The author’s personal preference, at least at this time, is to apply a separate zirconia primer (Z-Prime, BISCO) after sandblast- ing when cementing zirconia restorations with a RMGI. The author also recommends a warm air dryer be used to evaporate
primer solvents from the zirconia surface after primer application. Warm/dry air is simply very effective at removing solvent carriers and by “heating up” the substrate one can speculate that reaction rates will be accelerated, molecular interactions become more frequent, and greater num- bers of chemical bonds are formed.
In situations where there is a lack of resistance and retention form, esthetics is an issue, or maximum adhesion is re- quired, then self-etching self-priming resin-based cements (i.e. RelyX Unice- m/3M ESPE, Maxcem/Kerr, Bis-Cem/ BISCO, G-Cem/GC) or resin-based cements used in conjunction with a den-
tin bonding agent (i.e. Duo-Link/BIS- CO, RelyX Ultimate Adhesive Resin Cement/3M ESPE, Multilink/Ivoclar) are preferable over conventional ce- ments. Resin-based cements have a dis- tinct advantage over RMGI and other conventional cements when it comes to bonding restorations on, or in, minimal- ly retentive preparations as they bond more durably and predictably to both tooth tissues and zirconia. In addition, they may be a better choice when dealing with translucent zirconia or zirconia res- torations with minimal occlusal thick- ness as resin-based cements allow better stress distribution when loaded, may in-
hibit crack formation, and generally op- timize overall assembly strength.25 On the downside, resin-based cements can be difficult to clean, are more technique sensitive, and require extra steps when used in conjunction with a separately placed bonding agent. While dual cure self-etching self-priming resin cements are popular with dentists because they do not require a separate bonding agent be placed on the tooth, dentists should be aware that the highest bond to tooth structure is achieved by the use of res- in cements used in conjunction with a separately placed bonding agent.

In fact, some studies have found that even the self-etching/priming cements (such as Unicem 2) that are designed to be used without a separate bonding agent per- form better, in terms of bond strength to tooth structure, when a separate bond- ing agent is placed on the tooth first.37-39 There is some ambiguity as to the neces- sity of using a separate zirconia primer with some resin-based cements. This is because some self-etching resin cements such as Panavia SA Cement (Kuraray) and Unicem 2 (3M ESPE) already con- tain a phosphate ester zirconia primer inherent in their formulations. This may preclude the need for a separate dedicated zirconia primer. Indeed, some of these materials have shown promise bonding to both tooth tissues and zir- conia without using a separately placed adhesive or primer.40,41
CONCLUSION
A misconception held by many dentists is that “you cannot bond to zirconia.” The fact is you can bond very predictably and durably to zirconia surfaces using a com- bination of sandblasting, a phosphate ester primer such as 10-MDP, and an appropriate resin-based cement42-46 (Figs. 11-14).
The optimal way to treat zirconia and tooth surfaces prior to placement of zirconia restorations is contingent on many factors including, the specific clinical conditions, how retentive the preparation is, the nature of the conventional or resin-based cement being used, the minimum occlusal thickness, whether the dentist or the lab sandblasted the zirconia, the type of zirconia being placed (conventional vs. translucent), and esthetics (will the color of the cement affect the esthetic result). Proper management of both the zirconia substrate and tooth tissues is crucial for predictable and du- rable clinical outcomes. As a general rule the intaglio surface of all zirconia resto- rations be particle abraded (sandblasted) and a zirconia primer placed (typically a phosphate ester such as 10-MDP).
However, this is not true in every situation, and the use of a separate zirconia primer is contraindicated or not necessary with some materials. In this regard manufac- turer instructions and recommendations should be followed precisel for optimal results. It is incumbent on all clinicians to familiarize themselves with optimal cementation options and pro hen placing zirconia restorations.
About Dr Gary Alex, DMD
Dr. Alex attended Penn State University on an athletic scholarship where he graduated with a degree in Biology in 1977. He then took advanced level graduate courses in chemistry and biology before working at Jefferson Hospital in Philadelphia. He attended Tufts University Dental School where he earned his DMD in 1981. He has taken thousands of hours of continuing dental education over the last 35 years with an emphasis on occlusion, adhesion, comprehensive dentistry, materials, and esthetics.
Dr. Alex has researched and lectured internationally on adhesive and cosmetic dentistry, dental materials, comprehensive dentistry, and occlusion. He is an accredited member of the American Academy of Cosmetic Dentistry and past president of the AACD New York Chapter. With a background in chemistry and adhesive technology, he is a consultant for numerous dental manufacturers and member of the IADR (International Association of Dental Research). He has written and had published numerous scientific articles and papers and regularly conducts and participates in scientific studies on materials and adhesives. He has studied occlusion extensively with Dr. Peter Dawson (Center for Advanced Dental Study) and the late Dr. Bob Lee (Lee Institute) and is a member of the AES (American Equilibration Society). He has been the director of “PAC Live Ultimate Occlusion” and “Aesthetic Advantage Occlusion and Comprehensive Dentistry” programs. He is co-founder of the “Long Island Center for Advanced Dentistry” which provides the advanced continuing education training for dentists through lecture and hands-on programs. Dr. Alex is on the editorial board of, and has had a number of articles published in, the highly respected and peer-reviewed publications “Inside Dentistry“, “Compendium”, “Journal of Cosmetic Dentistry”, and “Functional Esthetics and Restorative Dentistry”. Dr. Alex is involved with a number of continuing education programs and regularly conducts hands-on programs and lectures on adhesion, porcelain veneers, direct and indirect restorations, materials, and occlusion. Dr. Alex maintains a busy fee for service practice in Huntington, NY, that is geared toward comprehensive prosthetic and cosmetic dentistry.
Zircon Lab is America’s leading dental lab. We are partnered with dental offices nationwide and are consistently growing. As America’s highest quality dental lab with the most competitive pricing, the highest caliber of product, expert craftsmanship, and fastest delivery, we set the dental industry standard. After choosing Zircon Lab to be your dental lab of choice, you can trust our dental product will be unmatched by any competitors.
References
- Makhija SK, Lawson NC, Gilbert GH, et al. Dentist material selection for single-unit crowns: findings from the National Dental Practice-Based Research Network. J Dent. 2016;55:40-47.
- Fischer J, Stawarczyk B, Hämmerle CH. Flexural strength of veneering ceramics for zirconia. J Dent 2008;3 6:316 – 321.
- Matsuzaki F, Sekine H, Honma S, Takanashi T, Furuya K, Yajima Y, Yoshinari. M. Translucency and flexural strength of monolithic translucent zirconia and porcelain-layered zirconia. Dent Mater 2015;34(6):910-917.
- Kayahan ZO. Monolithic zirconia: A review of the literature. Biomedical Research 2016;27(4):1427-1436.
- Ritzberger C, et al. Properties and Clinical Application of Three Types of Dental Glass-Ceramics and Ceramics for CAD-CAM Technologies. Materials 2010;3:3700-3713.
- Burgess JO, et al. Enamel Wear Opposing Polished and Aged Zirconia. Op Dent 2014:39(2):189-194.
- Daou EE. Esthetic Prosthetic Restorations: Reliability and Effects on Antagonist Dentition. Open Dent J 2015;9:473-481.
- Esquivel-Upshaw JF, et al. Randomized clinical study of wear of enamel antagonists against polished monolithic zirconia crowns. J Dent 2018 Jan;68:19-27.
- Piconi C, et al. On the fracture of a zirconia ball head. J Mat Science: Materials in Medicine 2006;17:289-300.
- Chevali J. What Future for Zirconia as a Biomaterial? Biomaterials 2006 (Feb);27(4):535-543
- Brown SS, Green DD, Pezzotti G, Donaldson T K, Clarke IC. Possible triggers for phase transformation in zirconia hip balls. J. Biomed. Mater 2008;85(2): 444-452.
- McLaren EA, Lawson N, Choi J, et al. New high-translucent cubic-phase-containing zirconia: clinical and laboratory considerations and the effect of air abrasion on strength. Compend Contin Educ Dent. 2017;38(6):e13-e16.
- Burgess J, et al. When Placing Zirconia or Lithium Disilicate Restorations, want factors govern your decision to employ traditional cementation or bonding protocols? Inside Dent August 2018 pages 52-53.
- Kwon SJ, Lawson NC, McLaren EE, Nejat AH, Burgess JO. Comparison of the mechanical properties of translucent zirconia and lithium disilicate. J Prosthet Dent. 2018 Jul;120(1):132-137.
- Kim BK, Bae HE, Shim JS, et al. The influence of ceramic surface treatments on the tensile bond strength of composite resin to all-ceramic coping materials. J. Prosthet. Dent. 2005;94:357–362.
- Yi YA, Ahn JS, Park YJ, et al. The Effect of Sandblasting and Different Primers on Shear Bond Strength Between Yttria-tetragonal Zirconia Polycrystal Ceramic and a Self-adhesive Resin Cement. Operative Dentistry: January/February 2015;40(1):63-71.
- Barragan G, Chasqueira F, Arantes-Oliveria S, Portugal J. Ceramic repair: influence of chemical and mechanical surface conditioning on adhesion to zirconia. Oral Health Dent Manag. 2014;13(2)155-158.
- Zandparsa R, et al. An in-vitro comparison of shear bond strength of zirconia to enamel using different surface treatments. J Prosthodont 2014;23(2):117-123.
- Zhang Y, Lawn BR, Rekow DE, Thompson VP. Effect of sandblasting on long-term performance of dental ceramics. J Biomed Mater Res B Appl Biomater. 2004;71(2):381-386.
- Chintapalli RK, Marro FG, Jimenez-Pique E, Anglada M. Phase transformation and subsurface damage in 3Y-TZP after sandblasting. Dent Mater. 2013;29(5):566-572.
- Ozcan M, Melo R, Souza RO, et al. Effect of air-particle abrasion protocols on the biaxial flexural strength, surface characteristics and phase transformation of zirconia after cyclic loading. J Mech Behav Biomed Mater. 2013;20:19-28.
- Alex G. Universal Adhesives: The next evolution in adhesive dentistry? Compendium 2015;36(1):15-28.
- Hallmann L, et al. Effect of blasting pressure, abrasive particle size and grade on phase transformation and morphological change of dental zirconia surface. J Prostet Dent 2016;115(3): 341-349.
- Personal communication Dr. Nasser Barghi (The University of Texas Health Science Center at San Antonio Dental School at San Antonio, Texas), Dr. Byoung Suh (Chemist and president BISCO Inc).
- McLaren E, Burgess J, Brucia J. Cubic-Containing zirconia: Is adhesive or conventional cementation best? Compendium 2008;39(5):282-284.
- Nagaoka, N. et al. Chemical interaction mechanism of 10-MDP with zirconia. Sci. Rep. 2017;30(7):45563; doi: 10.1038/srep45563.
- Xubiao L, et al. Enhancement of Phosphate Adsorption on Zirconium Hydroxide by Ammonium Modification. Industrial & Engineering Chemistry Research 2017 56 (34), 9419-9428.
- Yang B, Lange-Jansen HC, Scharnberg M, et al. Influence of saliva contamination on zirconia ceramic bonding. Dent Mater.2008;24(4):508-513.
- Chen L, Suh BI, Shen H. Minimize the contamination of zirconia restoration surface with saliva [abstract]. J Dent Res. 2013;92(spec iss A). Abstract 1654.
- Khan AA, et al. Recent Trends in Surface Treatment Methods for Bonding Composite Cement to Zirconia: A Review. Journal of Adhesive Dentistry 2017;19(1):7-19.
- Alex G. Preparing porcelain surface for optimal bonding. Compend Contin Educ Dent 2008;29(6):324-335.
- Information confirmed via E-Mail with Dr. Jesper Loof Tekn, CEO and Executive VP Operations and Research and Deveopement–Doxa Dental.
- Alnassar T, Ozer F, Chiche G, Blatz MB. Effect of different ceramic primers on shear bond strength of resin-modified glass ionomer cement to zirconia. J Adhesive Science and Tech 2016;30(22):2429-2438.
- Liang Chen PhD–Head Chemist, BISCO Inc.–Personal communication.
- Kobes KG, Vandewalle KS. Bond strength of resin cements to zirconia conditioned with primers. Gen Dent. 2013;61(6):73-76.
- Clinicians Report (CR) 2018;11(3):1-3.
- Barcellos DC, Batista GR, Silva MA, et al. Evaluation of bond strength of self-adhesive cements to dentin with or wihout application of adhesive systems. J Adhes Dent. 2011;13(3):261-265.
- Chen C, He F, Burrow MF, et al. Bond strengths of two self-adhesive resin cements to dentin with different treatments. J Med Biol Eng. 2011;31(1):73-77.
- Pisani-Proença J, Erhardt MC, Amaral R, et al. Influence of different surface conditioning protocols on microtensile bond strength of self-adhesive resin cements to dentin. J Prosthet Dent. 2011;105(4):227-235.
- Koizumi H, Nakayama D, Komine F, et al. Bonding of resin-based luting cements to zirconia with and without the use of ceramic priming agents. J Adhes Dent. 012;14(4):385-392.
- Personal conversation via Email with Dr. Reinhold Hecht, Division Scientist–Research & Development, 3M Oral Care.
- Yi YA, Ahn JS, Park YJ, et al. The effect of sandblasting and different primers on shear bond strength between yttria-tetragonal zirconia polycrystal ceramic and a self-adhesive resin cement. Oper Dent. 2015 Jan-Feb;40(1):63-71.
- Barragan G, Chasqueira F, Arantes-Oliveria S, Portugal J. Ceramic repair: influence of chemical and mechanical surface conditioning on adhesion to zirconia. Oral Health Dent Manag. 2014;13(2)155-158.
- Zandparsa R, Talua NA, Finkelman MD, Schaus SE. An in-vitro comparison of shear bond strength of zirconia to enamel using different surface treatments. J Prosthodont. 2014;23(2):117-123.
- Kern M. Bonding to oxide ceramics-laboratory testing versus clinical outcome. Dent Mater. 2015;31(1):8-14.
- Tanis MC, Akay C, Karakis D. Resin cementation of zirconia ceramics with different bonding agents. Biotechnology & Biotechnological Equipment 2015;29(2):363-367.

Recent Comments